Regain Control. Live Confidently.
Effective, modern treatment options for mixed urinary incontinence (stress + urgency).
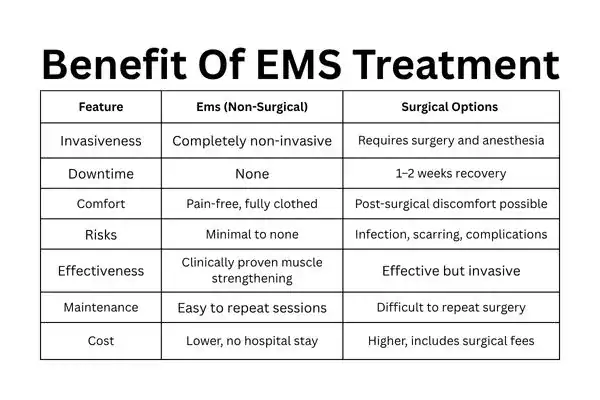
Whether you leak when you cough, laugh or have sudden, urgent trips to the bathroom, there are non-surgical and surgical options — including a cutting-edge, non-invasive electromagnetic therapy called EMS.

Mixed urinary incontinence (MUI) is leakage that has characteristics of both stress urinary incontinence (SUI) — leakage with physical exertion — and urgency urinary incontinence (UUI) — leakage associated with an acute, unprompted urge. Management typically begins with conservative measures (lifestyle changes and pelvic-floor muscle training) and progresses to devices or surgery when symptoms remain.
Conservative first: First-line choices are bladder training and supervised pelvic-floor muscle training (PFMT).
Non-invasive: device-based HIFEM therapies (such as EMS) increase pelvic-floor strength without invasive ut probes or significantly invasive surgery. Data supporting improvement in SUI, UUI and mixed symptoms have been reported for many of these patients.
Surgical: mid-urethral slings and other surgeries work for SUI and induce lasting symptom improvement, but they are invasive with the consequences of surgical risk and recuperation time. Data from clinical guidelines and RCTs with long-term follow-up suggest even greater reductions in long-term symptom levels among selected surgical patients.
The EMS chair treatment uses electromagnetic energy to trigger powerful pelvic floor muscle contractions, helping women of all ages to strengthen their pelvic floor muscles and pelvic muscles, improve bladder control, and reduce urine leaks caused by stress incontinence, urge incontinence, or pelvic organ prolapse—supporting daily activities and overall confidence, while addressing individual needs, minimising dependence on incontinence products, and being guided safely through every step of the way with awareness of any possible risks; complementing traditional pelvic floor exercises and care for related medical conditions.
EMS uses pulsed electromagnetic fields (HIFEM) delivered through a chair to stimulate pelvic-floor neuromuscular tissue and cause involuntary, supramaximal pelvic-floor muscle contractions. Those contractions are intended to improve muscle strength and neuromuscular control — similar in effect to many Kegel exercises but performed non-invasively. Clinical trials and device evaluations report improvements in the frequency of leakage episodes and quality of life for many patients.
EMS is cleared by the FDA (510(k)) for the treatment of urinary incontinence; it’s generally well-tolerated. Contraindications commonly include pregnancy, implanted electronic devices (e.g., pacemaker, ICD), certain metallic pelvic implants and active pelvic infection. Muscle soreness and tingling are common, mild, and temporary side effects.
As with any therapy, discuss medical history and devices with your clinician.
Overactive bladder is one of the most frequently observed types of urinary incontinence, causing a sudden urge to urinate, urine leakage and disruption to daily life — specifically in people with weak pelvic floor muscles, limited mobility or other health conditions that affect the urinary tract or bowel function.
Age-related problems with the pelvic floor, hormonal changes and the physical consequences of overactive bladder syndrome, overflow incontinence or accidental leakage of urine when the bladder is full during bowel movement can all be treated through pelvic floor muscle training, specialist nurses or electromagnetic technology—all effective solutions that have been proven to improve sexual health and overall quality of life, countering social isolation while safely addressing various concerns about types of urinary incontinence accompanied by advice on dealing with potential risks, litres/frequency/what now poops-volume/intake pressure requirements or any further questions regarding one’s specific type urinary incontinence prior.
Q: Is EMS FDA-cleared?
A: Yes — EMS has 510(k) FDA clearance for treating urinary incontinence and is widely used in clinics; manufacturers and regulatory documents confirm clearance. Like any other medical device, have your clinic provide its regulatory and clinical documentation.
Q: How many sessions will I need, and how long do they last?
A: Normal courses are 8-10 sessions (around 28–30 minutes each), typically run 1–2 times per week. You should customise the plan with your clinician.
Q: Is it painful?
A: According to a review by Lim and colleagues, although some studies have reported positive effects of magnetic stimulation for urinary incontinence, the overall evidence is inconsistent and more research is needed to fully understand patient experiences and outcomes.
Q: When will I start to feel better?
A: It varies; some people have improvements after the first few sessions and some take the entire course. The immediate and long-term benefit varies by individual and symptom type. Many participants are reporting improvements in their symptoms and quality of life, the trials found.
Q: Are there people who should NOT have EMS?
A: Yes — contra-indications commonly include pregnancy, implanted electrical devices (e.g., pacemaker/ICD), metallic pelvic implants, and active pelvic infections. Always review full medical history and implants with your provider.
Q: Can EMS replace surgery?
A: It can be an effective non-surgical option for many patients and may reduce or eliminate symptoms for some.